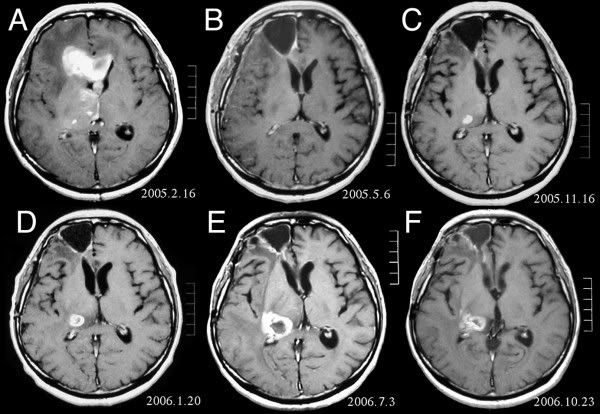
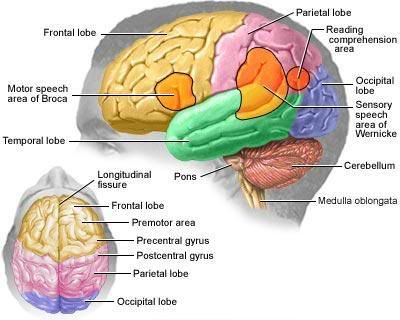
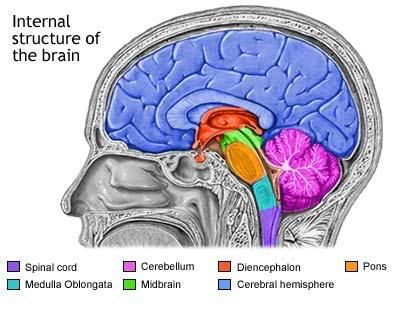
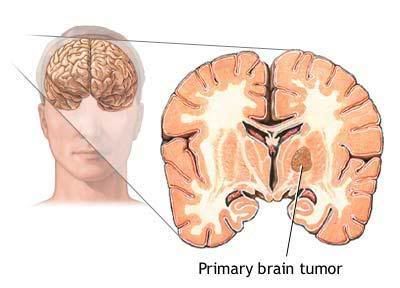
- Where inside my brain is the cancer located and where will it spread?
- What types of treatment are recommended?
- What are the possible side effects of this treatment?
- How can the side effects be minimized?
- Am I eligible for any clinical trials?
- Are there any alternatives to this treatment?
- What are the chances that the cancer will return?
- Will this cause any disabilities?
- How will this affect my daily life?
Often GBM cannot be entirely surgically removed because it affects large areas of the brain. Radiation therapy will be given regardless of whether surgery is possible, except to very young children. Conventional radiation may be performed, but more specialized types, such as stereotactic radiosurgery, which uses imaging and a computer to treat the tumor very precisely, or interstitial radiation, which delivers radiation by placing radioactive material directly on the tumor, may also be used. Chemotherapy will follow radiation; it may include carmustine, lomustine, procarbazine, and vincristine.
GBM is most common in patients over 50 years of age and rarely occurs in patients under 30. Increasing age is associated with a poorer prognosis. Median survivalis 9 to 11 months following treatment. Fewer than 5% of patients are alive five years later. Because of the poor prognosis of GBM, it is treated more aggressively than low-grade astrocytomas; many clinical trials take place to test new treatments.
Alternative and complementary therapies
While no specific alternative therapies have become popular for this particular type of brain cancer, patients interested in pursuing complementary therapies should discuss the idea with their doctor. A doctor may be able to provide information about the efficacy of certain techniques and whether they may interfere with conventional treatment.




0 comments:
Post a Comment